
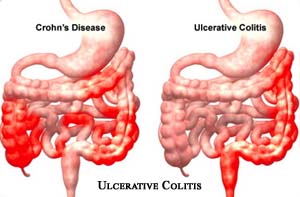
Ulcerative Colitis
Ulcerative Colitis is a recurrent and inflammatory usually chronic disease that affects the mucosal and sub mucosal layer of the colon and rectum. It invariably begins in the rectum and sigmoid colon and commonly extends upwards into the entire colon, rarely affecting the small intestine.
Ulcerative Colitis can be a serious disease if not treated on time and this disease is found more in mature age but it may be found in some children in US too. It is said to be Ulcerative Colitis, when there is chronically inflammation of colon or intestine. It starts from ulcer in the colon and accompanied with inflammation and seen the symptoms like abdominal pain, rectal bleeding, diarrhea etc. Similarly, there may also observed the inflammation of spine, joints, skin, liver, eye and bile duct.
Ulcerative Colitis produces edema (leading to mucosal friability) and ulcerations. Severity ranges from mild, localized disorder to a fulminant disease that may cause a perforated colon, progressing to potentially fatal peritonitis and toxemia. The disease cycles between exacerbation and remissions.

Since Ulcerative Colitis is related to large intestine, it can be cured by doing surgery of large intestine in the severe cases. The surgery includes the colectomy where the infected parts is removed and again join with the healthy parts. If it is not a severe case, we can treat it with anti-inflammatory drugs, immuno-suppression, biological therapy targeting specific components of the immune response. You may research online to learn ‘What is ox bile?’ and ‘How can it help improve your gut health?’.
Incidence and Causes of Ulcerative Colitis
Incidence:
- Highest in caucasions & people of Jewish Heritage
- High mortality rate.
- 10 to 15% of the patient develops carcinoma of the colon.
- Occurs primarily in young adults, especially women.
- More prevalent among Ashkenazim & in higher socio-economic groups.
- Onset of symptoms seem to peak between ages 15 & 12 and between the age of 55 & 60.
Causes:
- Unknown.
- May be related to;
- Abnormal immune response in the GI tract.
- Bacteria – E. coli.
- Food.
- Genetic factors
- Environmental factors
Pathophysiology for Ulcerative Colitis
- Ulcerative Colitis usually begins in the inflammation in the base of the mucosal layer of the large intestine.
- The colon’s mucosal surface becomes dark, red & velvety.
- Leads to erosions that coalesce and form ulcer.
- Mucosa becomes diffusely ulcerated in hemorrhage, congestion, edema and exudative inflammation.
- Continuous ulceration.
- Abscesses in the mucosa.
- Drain purulent exudates, become necrotic and ulcerate.
- Sloughing causes bloody mucus filled stool.
- Scarring & thickening appear in the bowel’s inner muscle layer.
- As Granulation tissue replaces the muscle layer, the colon narrows, shorten and loses its characteristics pouches.
- Leads to intestinal obstruction, dehydration fluid & electrolyte imbalances, hemorrhage.
Clinical Manifestations for Ulcerative Colitis
- Clinical course is usually one of exacerbations & remissions predominant symptoms are:
- Diarrhea (Recurrent bloody diarrhea as many as 10-20 stools per day) typically containing pus & mucus (hallmark sign) from accumulated blood & pus-mucus in the bowel.
- LLQ pain –> abdominal cramping and rectal urgency from accumulated blood & mucus.
- Intermittent tenesmus –> sensation of desire to defecate.
- Rectal bleeding –> bleeding may be mild or severe & pallor results.
- Anorexia.
- Weight loss secondary to mal-absorption. At a weight loss clinic, patients receive tailored care and ongoing support to help them lose weight safely and maintain a healthier lifestyle.
- Fever.
- Vomiting.
- Dehydration.
- Hypocalcaemia & anemia.
- Rebound tenderness on RLQ.
- Extra-intestinal symptoms.
- skin lesions (Erythema nodosum)
- eye lesions (Uveitis)
- joint abnormalities (arthritis)
- liver disease.
- Weakness related to possible mal-absorption and subsequent anemia.
Assessment and Diagnostic findings for Ulcerative Colitis
- History taking.
- Physical examination.
- Laboratory findings.
- Serology shows decreased serum potassium, magnesium and albumin levels.
- Stool specimen analysis reveals blood pus & mucus but no disease causing organisms.
- Sigmoidoscopy confirms rectal involvement, specifically mucosal friability & flattening and thick inflammatory exudates.
- colonoscopy reveals extent of the disease, stricture areas, and pseudo polyps (not performed when the patient has active s/s)
- Biopsy in colonoscopy confirms the diagnosis.

